
What is Carpal Tunnel Syndrome?
CTS is the most common condition affecting the hand in the western world. It affects 10% of the working and non-working population. CTS is caused by compression of the median nerve at the wrist. Compression of a nerve causes decreased blood flow, which reduces nutrient and oxygen supply to the nerve, causing disturbances in nerve conduction.
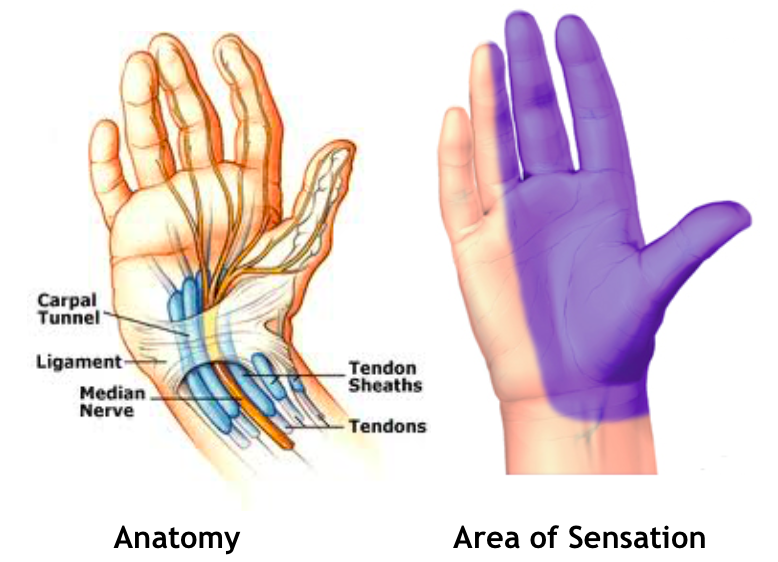
The carpal tunnel is a channel formed by bone and a tough ligamentous structure (transverse ligament) at the wrist at the heel of the hand. Through this rigid tunnel passes nine tendons that bend the fingers, connective tissue, arteries, veins, and the median nerve. The median nerve gives sensation and muscle control to the palm side of the thumb, index finger, middle finger and one half of the ring finger. The median nerve activates the small muscles of the thumb to oppose the thumb to the other fingers.
When swelling develops in the carpal tunnel or when the carpal tunnel becomes compressed, pressure is placed on the median nerve which leads to pain, numbness and pins and needles mostly at night, causing waking. If compression on the nerve is prolonged symptoms can progress to include numbness during the day, muscle wasting causing loss of function such as clumsiness and weakness of grip and pinch that may be irreversible
The 3 major predisposing factors to the development of CTS are being female, middle aged and obese. Others include:
- Systemic disorders – diabetes, rheumatoid arthritis, hypothyroidism.
- Tenosynovitis – thickening of the synovium (covering of the tendons) caused by overuse/ friction of the tendons. Common in those with Rheumatoid Arthritis.
- Odema – increased fluid within the carpal tunnel, e.g. pregnancy, tissue injury.
- Fractures, dislocation of the wrist – displaced bones disrupt the carpal tunnel.
- Abnormal structure protruding into the carpal tunnel – ganglion, bony spur, abnormal muscle belly, displaced fracture.
Management of Carpal Tunnel Syndrome
The goal is to decrease pressure on the median nerve. If diagnosed early, can prevent permanent damage over time.
- Wrist Splint: Decrease compressive wrist positions
- Anti inflammatory medication
- Activity modification: If repetition is unavoidable, keep the wrist in a neutral position when hands are in motion. Discontinue activity if it causes pain.
- Cortisone Injection or iontophoresis
- Neck assessment: Your therapist will refer you to a Physiotherapist for a Cervical Spine assessment if there is concern of compression at a higher level.
- Surgical referral: Your therapist will advise you if your symptoms require referral to a Plastic Surgeon.
- Avoid high salt intake as causes water retention, and Smoking which reduces blood flow.